
Medical Progress
Image courtesy of Library and Archives Canada
During the First World War new weaponry, including tanks, chlorine gas, and machine guns led to millions of deaths and injuries. Poor living conditions in the trenches and disease also contributed to these high casualty rates. For example, medical staff performed over 40,000 amputations on British troops, including over 3000 members of the Canadian Expeditionary Force. Many of the amputations were a result of infections in the trenches.
Treating the Wounded
Examine the following chart to see the process of treating an injured soldier.
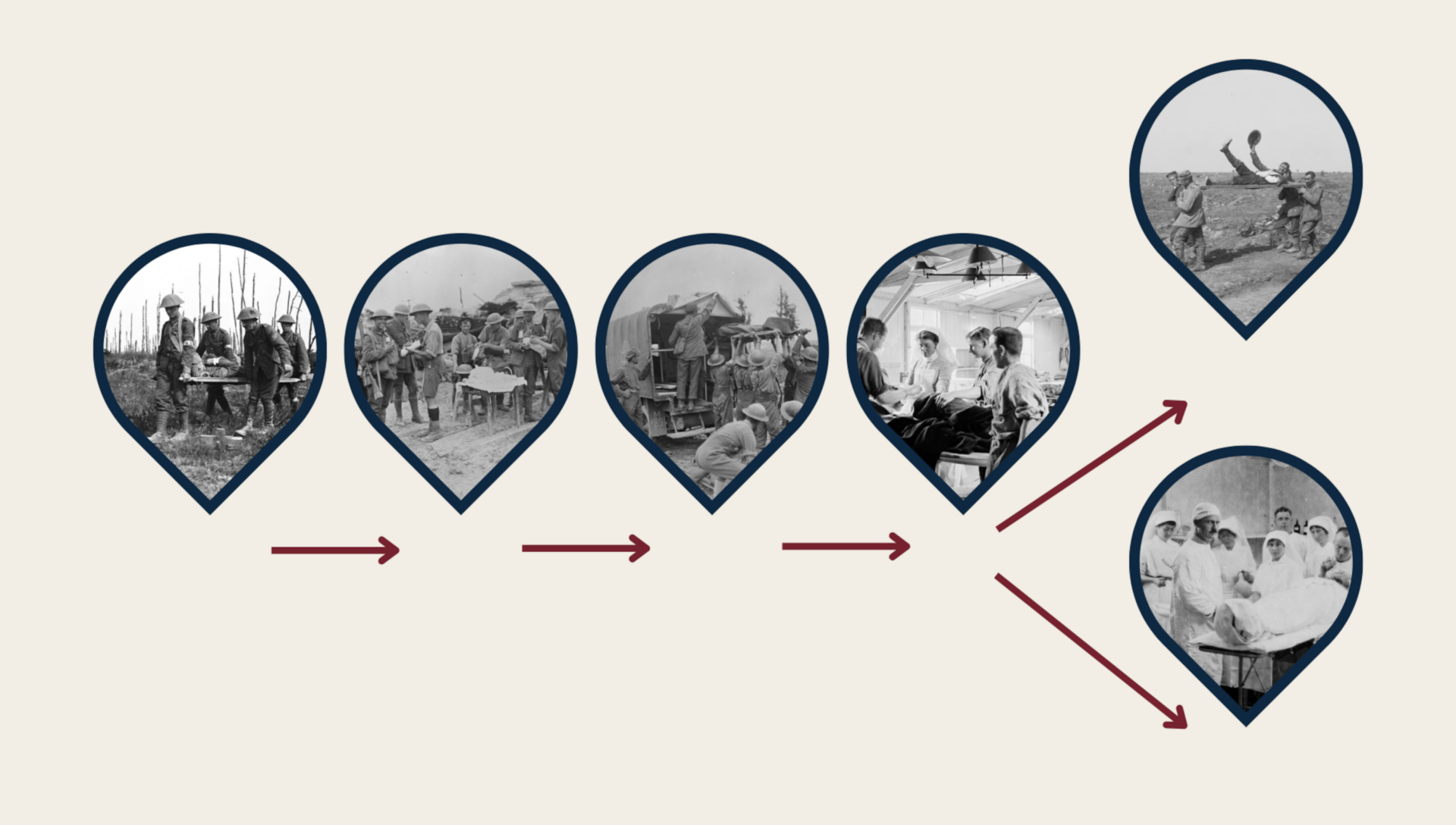
images courtesy of Library and Archives Canada and the Imperial War Museums.
Innovation on the front
The need for medical advances to treat and prevent casualties led to numerous medical innovations that are still used today. Anesthesia, antiseptic, blood transfusions, facial reconstructive surgery, and portable x-ray machines were all born out of the necessity to treat the millions injured by the violence and devastation of the war.
Think: How would the following medical advances affect the role of nurses on the front?
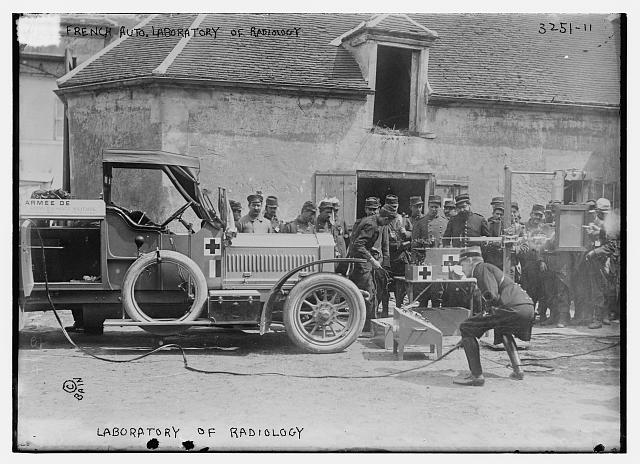
Even though several hospitals were equipped with X-ray machines by 1914, they were far from battlefields. Marie Curie, who won the Nobel Prize for her discovery of radium, and her daughter created radiology services for the military. They brought the X-ray machines directly to the front in cars converted into X-ray vans called “petites Curies”. This technology allowed doctors to scan wounds directly at the front. This technology saved many lives, as surgeons could remove the shrapnel and bullets seen in the x-rays.

The history of blood transfusions began in the early 1700s, but the practice at that time used erratic methods and produced poor results. As modern medicine developed in the early 1900s, a series of doctors began to explore the potential benefits of human blood transfusions. Prior to WWI, Dr. Edward Archibald in Montreal and Dr. Lawrence Bruce Robertson in Toronto independently took an interest in blood transfusions and began practicing with patients at their respective hospitals. At the onset of war, these two Canadians both enlisted and quickly realized the benefits of blood transfusions to patients who were hemorrhaging and in shock. These two men continued their efforts to advance the cause, and both published influential articles.
The following summer, with the arrival of the U.S. forces in 1917, American Dr. Oswald Hope Robertson was able to add his own research into the preservation of blood and its adaptation for blood transfusions on the battlefield. He created the first blood bank, using donated blood stored with sodium citrate as an anticoagulant. The combined research of these three doctors had a major impact not only on the war, but on the entire practice of medicine and surgery, the results of which are still important today.
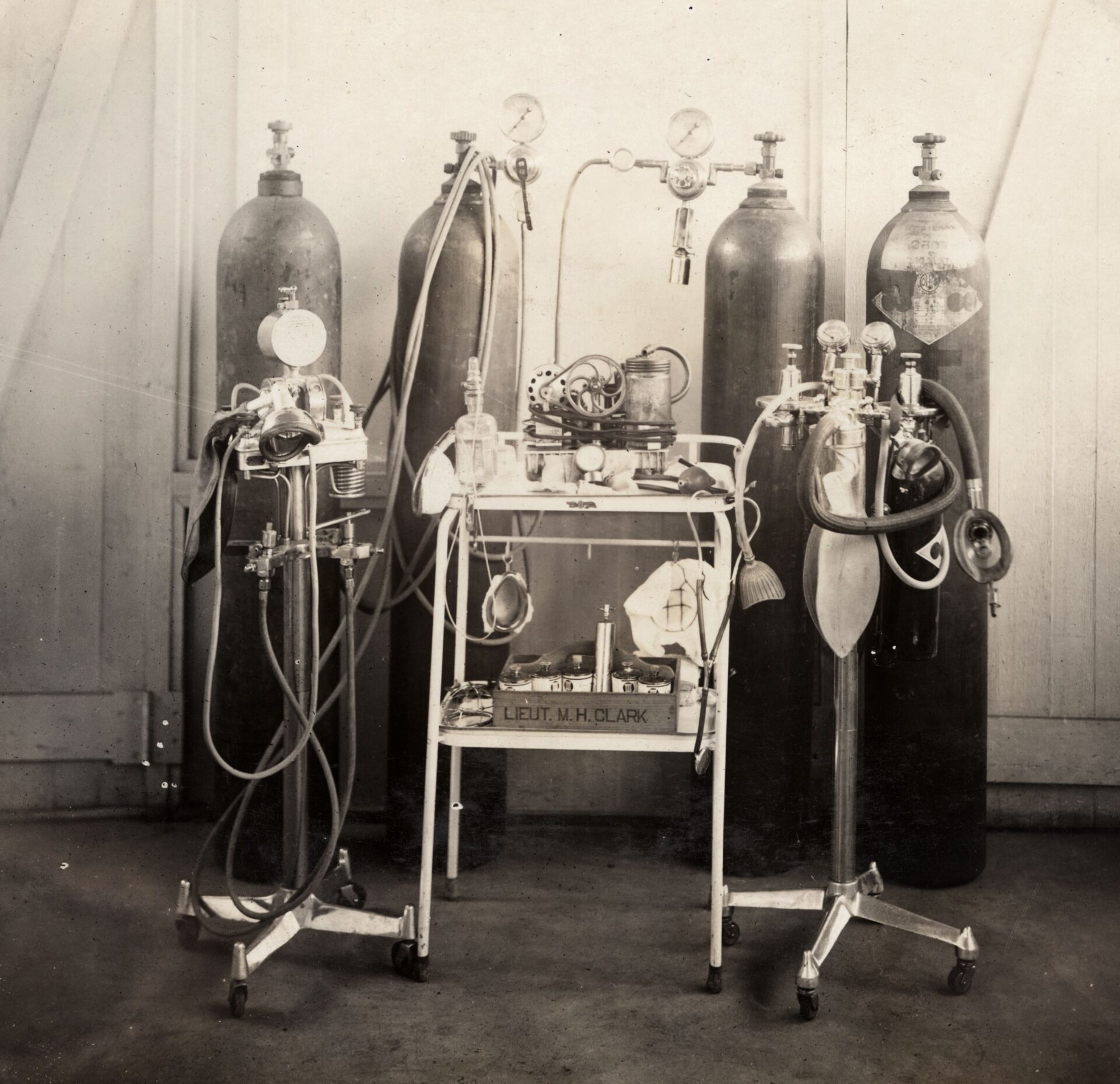
Anesthetic Equipment (National WWI Museum and Memorial, Kansas City, Missouri, USA).
At the start of WWI, the practice of anesthesia was an unstructured specialty with techniques and methods varying between institutions. During the war, the practice adapted and developed at an accelerated pace, becoming its own subspecialty for both physicians and nurses. Several leaders took note of the new developments and helped institutionalize changes, including Captain Arthur Guedel. Guedel helped define the stages of anesthesia and supported the education of anesthesiologists and nurses.
The creation of specialty posts for anesthesiologists also helped support research in blood transfusions and resuscitation, which were vital for preventing deaths and treating patients suffering from shock. In casualty clearing stations, essential nursing and surgical care worked at such a fast pace that staff combined analgesic gas treatments, which was not only better for the patients, but also eventually lead to the development of an anesthetic machine that could more accurately monitor and dispense treatments. Also, in 1915, at the American Ambulance Hospital, Dr. George Crile and nurse Agatha Hodgins showed their colleagues how to use a mixture of nitrous oxide and oxygen to anesthetize patients. This method would be used for reconstructive surgery, among other procedures.

The world of medical rehabilitation was forever changed with the invention of the first artificial leg by Benjamin Franklin Palmer in 1847. Wounds caused by artillery and subsequent gangrene infections caused many soldiers to lose limbs. Even though amputated soldiers would never fully recover, the use of prosthetic limbs greatly improved their mobility and quality of life. Nurses also served as physiotherapists for recovering soldiers learning to use their prosthetic limbs.

The war resulted in the development of several medications. For example, in 1915, Henry Dakin, a British biochemist, perfected a sodium hypochlorite solution, which killed dangerous bacteria without burning flesh. He used it to flush out and clean open wounds before they were closed off (either by stitching, burning, or amputation) to prevent infection. The technique became known as the “Carrel-Dakin Method” many doctors across Europe adopted the technique during the war. Morphine also became very popular and given to ease pain and to allow the badly wounded to die painlessly. Nurses were trained and ready to administer these antiseptics, anesthetics, and other medications when needed.
In a sense, nurses were trailblazers of mental healthcare. The care and comfort they provided allowed soldiers to speak up about the horrors that they witnessed on the battlefield. Some nurses had a background in social work and psychiatry, which gave them an edge for helping soldiers deal with their experiences.
Through their eyes
Jean Elizabeth Sword
Donating blood on the front

Biography
Born in Owen Sound, Ontario in 1893, Jean Elizabeth Sword enlisted in the war in September 1914. She worked in military hospitals in both France and England. On April 22, 1918, she acted as a blood donor for a soldier undergoing a blood transfusion. The donation left her weak, but she was able to recover and continue her work. In June 1918, she received the Royal Red Cross medal 2nd Class.
Madeleine Jaffray
Canada’s only female amputee of WWI

Biography
Madeline Jaffray was born in Chicago in 1889 and grew up in Galt, Ontario. After training as a nurse, she went overseas with the French Red Cross in 1915. While working at a mobile ambulance unit near Adinkerke, she was injured in the foot by shrapnel, which led to an amputation. She was Canada’s only
female amputee of the First World War. After returning home, she worked at the Christie Street Veterans Hospital in Toronto and was heavily involved with the WarAmps to help other amputees across Canada.
Alfreda Attrill
An early physiotherapist

Biography
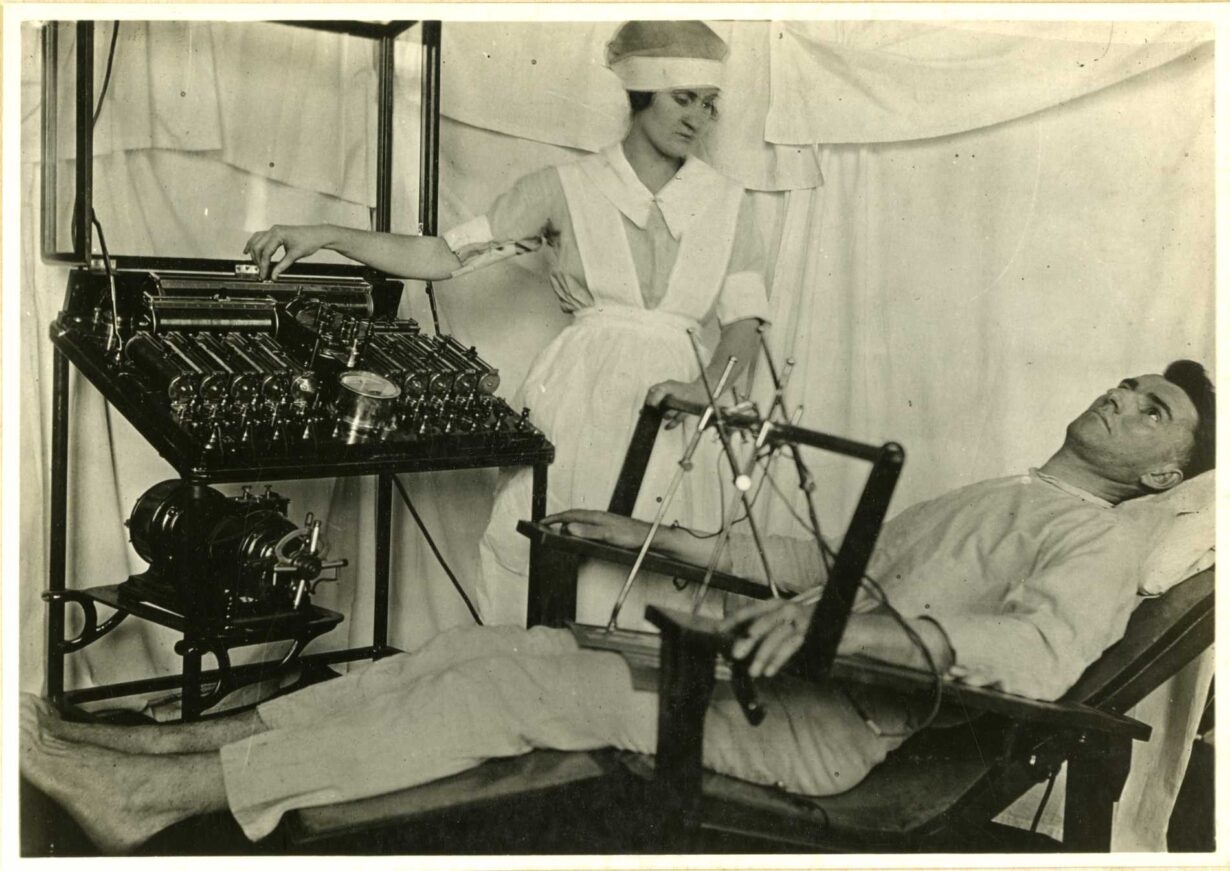
Alfreda Jean Attrill was born in Minden Ontario, in 1877. She originally studied to become a teacher but later enrolled at the Winnipeg General Hospital School of Nursing in 1906. In 1914 she went overseas and served in France, Salonika and England. In 1918, she took a three-month training course at the Granville Canadian Special Hospital in ‘military massage’. There she learned the basics of what today would be considered physiotherapy. She used the skills to help many patients during her service. After the war, she became an advisor for the Department of Health in Winnipeg. She was also very involved with the St. John’s Ambulance.






